The ITB – 5 things you probably haven’t thought about doing to help it
 Consider this patient: Sarah* is a 38yo female runner training for a half-marathon "fun run" develops pain over the outside of the knee. It hurts to stand up and sit down, especially after being in one position for a long time. Once she warms up, it doesn't hurt so much during the run but it will ache later. She has iced the knee, rolls on it with a foam roller, gets massage/ART on it, and does some banded sideways walking, clams and hip abduction strengthening exercises. She has a massage ball and dutifully attacks the overactive hip flexors and TFL muscles...but she isn't getting anywhere. She still basically has pain and it is getting worse and she can't up the miles as per her running program. She has seen another physio, a chiro, massage therapists and had some acupuncture. She drinks plenty of water and has her nutrition dialed in nicely. She has been given the diagnosis of ITBFS - Ilio-Tibial Band Friction Syndrome...Sound familiar?
Consider this patient: Sarah* is a 38yo female runner training for a half-marathon "fun run" develops pain over the outside of the knee. It hurts to stand up and sit down, especially after being in one position for a long time. Once she warms up, it doesn't hurt so much during the run but it will ache later. She has iced the knee, rolls on it with a foam roller, gets massage/ART on it, and does some banded sideways walking, clams and hip abduction strengthening exercises. She has a massage ball and dutifully attacks the overactive hip flexors and TFL muscles...but she isn't getting anywhere. She still basically has pain and it is getting worse and she can't up the miles as per her running program. She has seen another physio, a chiro, massage therapists and had some acupuncture. She drinks plenty of water and has her nutrition dialed in nicely. She has been given the diagnosis of ITBFS - Ilio-Tibial Band Friction Syndrome...Sound familiar?
In this blog post, I want to give you 5 things to think about that may just make the difference between getting better and not.
(*"Sarah" is not her real name)
 1. Muscles that directly attach onto (or touch) the ITB
1. Muscles that directly attach onto (or touch) the ITB
The 3 muscles that are most directly responsible for producing ITB tension are...
a. Gluteus Maximus (Glute Max) - a significant portion of this muscle attaches directly to the ITB
b.Tensor Fascia Lata (TFL) - This muscle works to help balance out the massive Gluteus Maximus attachment. It is often compensating for poor hip control
c. Vastus Lateralis (VL) - That's right. This massive quad muscle goes quite high and to the side and back of the thigh - higher and further around the side and back than most people think. Since the ITB directly sits and attaches to the tissue surrounding VL, contraction of this muscle will "bulge" and 'bow" the ITB
 2. Muscles that may indirectly affect the ITB
2. Muscles that may indirectly affect the ITB

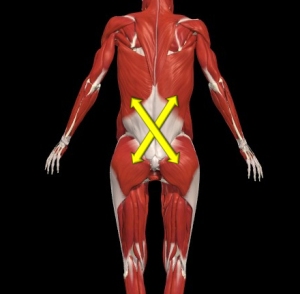
a. Contralateral Latissimus Dorsi (the lat on the other side of the sore ITB) can actually transmit force via the thoracolumbar fascia and Glute Max.
b. Tibialis Anterior - via the lateral retinaculum - this is not as strong as the relationship between the contralateral Lat Dorsi and Glute Max but still worth considering - I have had good success when the Tibialis Anterior tested as being involved and significant.

Tim Chalmers from CrossFit Creature demonstrating a bad position - note the hip adduction, hip internal rotation, knee is twisted (unbalanced muscular forces) and a bit of foot pronation.
3. Movements that can affect the ITB
These are more commonly known...but read carefully...maybe there is a small difference that can make ALL the difference
a. Hip Adduction on the stance leg. Often referred to as weak hip abductors causing the problem, investigate further. Sometimes it is simply a motor control problem. Other times it is because other factors (like another body region) causes a compensation at the hip. The Gluteus Medius and Minimus tends to work with the TFL to help control the pelvic position.
b. Hip Internal Rotation on the stance leg. Again, this is known and the cue "knees out" is used to counter this...but look for WHY the joint wants to internally rotate. The Deep Hip External Rotators (DHER) are Piriformis, Gemelli, Obturators as well as Quadratus Femoris - they all contribute towards rotational control of the hip. Gluteus Medius and Minimus have some rotational contribution as well
c. Knee muscular forces not balanced. These are things like the Gastrocs, Popliteus, Hamstrings and Quads via the Patella Tendon.
d. Foot Pronation
 4. Poor Femoral Head Centering
4. Poor Femoral Head Centering

This is a KEY issue. Solving this problem often solves lots of other problems. It isn't easy to do and you often need someone experienced to help you learn how to do it properly. Getting this right will change your life! Basically, think about someone having a hold of your leg and you are gently shortening the leg. That is usually a useful cue. Another is to feel behind the greater trochanter and feel it become "fuller" behind there. I will try to produce a video on it.
Some of the muscles that you want to work are Iliacus as well as the DHER as well as ensuring the hip posterior capsule allows the femoral head to glide posteriorly.
 5. Structural Issues
5. Structural Issues

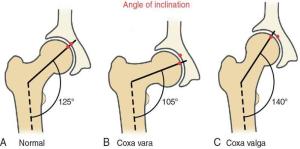
Hip dysplasia, femoral anteversion or retroversion, Cam Impingement, Pincer Impingement (or mixed presentation - both present), the angle of your acetabulae, the Q angle you have, your tibial torsion, your foot posture...all of these things and more can play a part in why you have altered mechanics of the hip. Add to that list of things all the things ABOVE the hips that can affect posture and position and there are lots of biomechanical and structural issues to consider.
A Simple Test
Stand on one leg and do a 1/4 squat while facing a mirror. Imagine you have a ping pong ball on each hip pointer bone...can you keep them level? Are you foot, knee and hip all in the one line?
If you can keep this alignment, you will need to do some work on getting control of the hip. Note, you will need the centre of your body to align with the inside of the foot to do this test and keep your balance.
A Simple Exercise
This is very similar to the simple test above:
a. Standing on the leg to be trained with the other foot behind you on the ground.
b. Get the alignment right in the mirror
c. Slowly drop into the 1/4 squat while keeping good alignment
d. Slowly take the weight off the back foot while keeping good alignment
e. Stand back up with good alignment - if you can take your foot off without losing alignment, then stand up on one leg.
f. Progress to starting with the other foot off the ground - remember, you must keep good alignment the whole time.
g. Ideally, you should be able to lower while taking the non-weightbearing leg behind you and stand up while taking that leg up in front (kind of mimics the motion of running a little).
Thanks to Tim Chalmers from CrossFit Creature for helping me out with the photos and videos. He had just completed a mammoth session and so he was a little tired demonstrating the exercises for me.
 Sarah's Story:
Sarah's Story:

So what did I do for Sarah?
First of all, I did all of the above - there was no injury or nerve problems to any of the muscles or joints involved or in the rest of the whole body screen I do, which just meant that she had some hip weakness, endurance and motor control problems to deal with. She had been doing some of the right exercises but she wasn't controlling the hip and pelvic position nor was she centering the femoral head (no one had taught her until I did). I checked her bony anatomy and apart from some slight torsions, there wasn't anything stopping her doing what she wanted to do...run a half marathon.
During my assessment, I used manual muscle testing and some tasks to show her how controlling the femoral head and pelvic position actually made it easier for her to control things and be "stronger". She then took those test-retest movements into her home program.
I started her on the simple test but also a few other standing/one leg exercises to teach her how to control the hip and pelvic position. I taught her to run keeping her pelvis level and slowly increased the distance and time and speed. She also had to squat full depth with either light weights or no weights
Within a few weeks, the ITB pain decreased significantly - basically it wasn't a problem and there was no more pain after running. She increased her miles slowly at first and when the strength and control were evident, she increased in bigger jumps without any problem - she was able to eventually catch up to her preparation for her half marathon and ran the fun run in a time she was happy with and without pain...a happy ending all around 🙂
 Summary:
Summary:

- Have a look at the muscles that directly affect the ITB and find out if you have to address them
- Have a look at the muscles that indirectly affect the ITB as per summary point 1.
- Can you control the movements of the hip and pelvis - there are lots of motor control issues with the muscles of the hip you can investigate
- Poor femoral head centering is a key component missed in hip rehab - I will try to produce a video on this very soon - subscribe to this blog to get the updates
- Consider your anatomy - perhaps the way you are built will mean that your ITB will tend to be put under pressure no matter how diligent you are. It doesn't mean you don't try to mitigate the effects of your anatomy...but understanding why it isn't perfect is a good thing.
- Use the simple test and exercise to get started on your rehab but you should go see someone to get it sorted.
If you would like an assessment with me (Antony Lo), just use the Email Contact Form below - I can do Skype consults as well as in-person consultations.
I would love to have an online discussion with you - please leave your comments on the blog by scrolling down lower and commenting at "Leave a Reply".
Email Contact Form
Error: Contact form not found.
Reblogged this on Minneapolis Personal Trainer.
Thank you!
Thanks very much Kel – there are plenty more articles on many different topics. Please feel free to have a look around and reblog anything else you find or just ask me to write a on a topic 🙂 Cheers!
Great article, thanks for sharing. I’ve had a lot of issues with my knee and now think it could be related to my hips. Looking forward to seeing the video on femoral head centering!